








28年的专注发展

其中发明专利15项

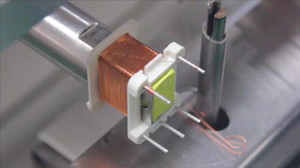
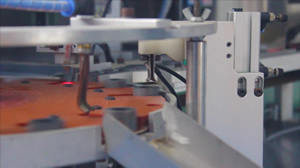
建成了5条精密互感器自动化生产线

荣获“湖北省守合同重信用企业”

分公司和销售机构












服务热线:400-086-3003
电话:0728-5353116 5353117
传真:0728-5353121
地址:湖北省天门市经济开发区创业大道8号